
The clitoral hood is one of the most misunderstood structures in female anatomy. It protects roughly 8,000 nerve endings, plays a direct role in arousal and orgasm, and varies significantly from person to person. Below, board-certified OB/GYN Dr. Sue Kafali separates six persistent myths from what current research actually shows.
Key Takeaways
- The clitoral hood protects nerve-dense tissue and plays a direct role in arousal, lubrication, and orgasm for most women.
- Hood size and shape vary widely and are influenced by genetics, hormonal shifts, childbirth, and conditions like lichen sclerosus.
- Research shows approximately 82% of women need some form of clitoral stimulation to reach orgasm, making hood anatomy more relevant than most people realize.
- Excess hood tissue can reduce sensation by creating a barrier between stimulation and the clitoral glans, but this is correctable.
- Clitoral hood reduction is the most commonly requested add-on to labiaplasty, often by patients whose first procedure left the hood untouched.
- Sensation preservation is a clinical priority when procedures are performed by a surgeon trained in female sexual anatomy and nerve pathways.
Why Clitoral Hood Anatomy Deserves More Attention
Most conversations about sexual health skip over the clitoral hood entirely. That’s a problem, because this small fold of tissue has an outsized impact on sexual function.
A 2018 study in the Journal of Sex & Marital Therapy surveyed over 1,000 American women and found that only 18.4% could orgasm from penetration alone. The remaining 81.6% reported needing clitoral stimulation. When the structure protecting those nerve endings isn’t discussed, a significant piece of the puzzle goes missing.
At FemSculpt, Dr. Kafali’s OB/GYN training means she approaches clitoral hood reduction with a deep understanding of how nerve pathways, blood flow, and tissue elasticity affect sensation. Preserving and improving sensation is a clinical priority, not an afterthought. That background matters, because it shapes every surgical decision from incision placement to the amount of tissue preserved.
What Is a Clitoral Hood?
The clitoral hood (also called the clitoral prepuce or “clit hood”) is a fold of skin formed by the upper junction of the labia minora. It partially or fully covers the glans of the clitoris, the small, highly sensitive external tip that contains approximately 8,000 nerve endings.
Think of it as a protective sleeve. The hood shields the clitoral glans from constant friction against clothing and allows the glans to remain sensitive to intentional touch during arousal. During stimulation, increased blood flow causes the clitoral structures to engorge, and the hood may retract slightly, exposing more of the glans.
Everyone’s hood is different. Some cover the glans completely, some partially, and some barely at all. There is no single “normal” appearance. The clitoral hood is embryologically homologous to the male foreskin. Both develop from the same tissue (the genital tubercle) during fetal development. This shared origin is one reason the hood contains such a dense concentration of nerve endings and responds to hormonal changes throughout life.
How the Clitoral Hood Relates to Orgasm and Sensation
The relationship between the clitoral hood and orgasm is more nuanced than “more exposure equals more pleasure.”
Clitoral anatomy influences orgasm likelihood. A 2022 study in the International Urogynecology Journal found that the distance between the clitoral glans and the urethra was a significant predictor of orgasm difficulty, independent of psychological factors.
The hood acts as a mediator. During arousal, the clitoral complex (which extends 9 to 11 cm internally, far beyond the visible glans) engorges with blood. The hood glides over the glans, providing indirect stimulation that many women find more comfortable than direct contact.
When excess hood tissue is present, this gliding mechanism becomes less effective. Too much tissue between the source of stimulation and the nerve endings may mute sensation. This doesn’t mean the nerves are damaged. It means the signal has a harder time getting through.
Hormonal changes add another layer. Hood tissue thickness and elasticity shift with estrogen and testosterone levels, meaning menopause, HRT, PCOS, and even hormonal birth control can change how the hood functions over time. Conditions like lichen sclerosus add further complexity by causing adhesions that restrict hood mobility.
6 Myths About the Clitoral Hood and Orgasm
Myth #1: All Clitoral Hoods Look the Same
Fact: Clitoral hoods vary enormously in size, shape, thickness, and coverage. A 2023 Clinical Anatomy meta-analysis confirmed substantial range across all clitoral structures. Your hood may fully cover the glans, partially cover it, or sit to one side. What matters is whether the anatomy is causing discomfort, reduced sensation, or distress.
Myth #2: A Larger Hood Always Means Less Sensation
Fact: Size alone doesn’t determine sensation. What matters is the relationship between your hood tissue and the underlying nerve endings. Some women with larger hoods have full sensation because the tissue is thin and mobile. Others with moderate hoods have reduced sensation because the tissue is thick or adhered. A cosmetic gynecologist evaluates tissue quality, mobility, and nerve response.
Myth #3: The Clitoris Is Just the Small External Nub
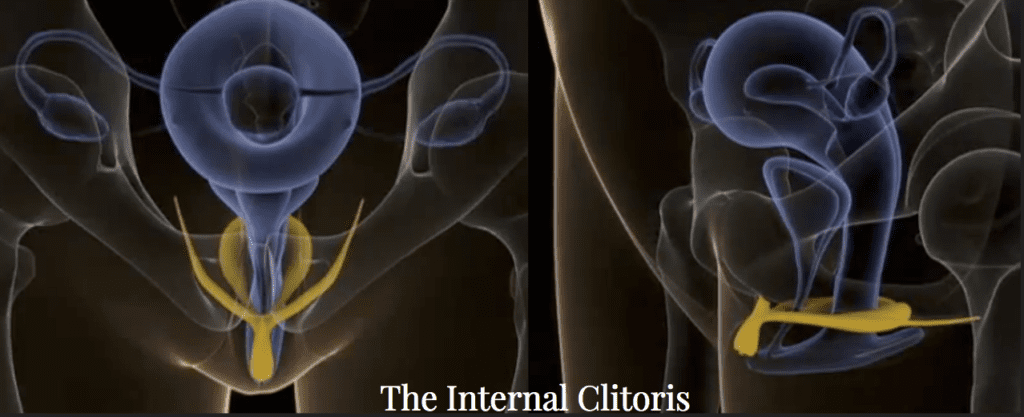
Fact: The visible glans is only the tip. The full clitoral complex includes the body, two crura (legs), and vestibular bulbs, totaling 9 to 11 cm. These internal structures surround the vaginal canal and engorge during arousal, which is why some women experience orgasm from internal stimulation. The hood protects the external gateway to this entire system.
Myth #4: Clitoral Hood Reduction Will Eliminate Sensation
Fact: This is the most common fear. But a prospective study in Plastic and Reconstructive Surgery (2015) tracked sensitivity before and after hood reduction using monofilament testing. At 12 months, no decrease in sensitivity was detected. 35.3% of subjects reported improved orgasm frequency and strength. The key is a surgeon who understands the dorsal nerve of the clitoris and preserves the critical 1 cm bridge of tissue that protects it.
Myth #5: Only Women Who’ve Had Children Need to Think About Their Hood
Fact: Many women have been self-conscious about excess hood tissue since adolescence. Others develop changes after hormonal shifts from menopause or medical conditions. Lichen sclerosus, a chronic inflammatory skin condition, can cause the hood to adhere to the clitoral glans (clitoral phimosis), reducing sensation independently of tissue volume. This affects women of all ages.
Myth #6: Orgasm Difficulty Is “All in Your Head”
Fact: Psychological factors play a role in sexual function, but anatomy matters too. Research shows approximately 75% of women do not reliably orgasm from penetration alone. The position, size, and coverage of clitoral structures directly influence how stimulation reaches the nerve endings responsible for orgasm. If you suspect a physical component, it’s worth a conversation with a specialist who understands clitoral anatomy.
When Excess Hood Tissue May Warrant a Consultation
Not every variation needs treatment. But there are situations where excess tissue or hood changes create real problems.
You may benefit from a consultation if you experience:
- Reduced sensation during intimacy that has worsened over time
- Visible excess tissue that causes self-consciousness or affects clothing comfort
- Irritation or chafing from the hood rubbing against clothing during exercise
- Difficulty with direct stimulation because the hood doesn’t retract enough during arousal
- Post-labiaplasty imbalance where the hood was left untouched
- Lichen sclerosus-related adhesions where the hood has fused to the glans
Hood reduction is the most commonly requested add-on to labiaplasty surgery. Many patients who had a previous labiaplasty elsewhere come to FemSculpt specifically because their first surgeon didn’t address the hood.
Consultations are $150 virtual or $250 in-person. Dr. Kafali evaluates your anatomy and discusses whether a procedure would meaningfully improve comfort, appearance, or sensation.
Non-Surgical vs. Surgical Options for Clitoral Hood Concerns
Not every concern requires surgery. Here’s a comparison of the most common approaches.
| Factor | Non-Surgical Options | Clitoral Hood Reduction (Surgical) |
|---|---|---|
| Best for | Mild adhesions, early lichen sclerosus, hormonal changes, sensation concerns without significant excess tissue | Excess hood tissue causing reduced sensation, cosmetic concerns, post-labiaplasty imbalance, moderate to severe coverage |
| Options include | Topical hormones (estradiol/testosterone), Climax Shot (O-Shot), Morpheus8V, pelvic floor therapy, lysis of adhesions (in-office) | Clitoral hood reduction, often combined with labiaplasty |
| Downtime | None to minimal (same-day return to normal activities for most) | About 1 week off work, 4-6 weeks before sexual activity |
| Results timeline | Gradual improvement over weeks to months | Visible results once swelling resolves (6-8 weeks), final results at 6 months |
| Sensation outcomes | May improve arousal and lubrication; less predictable for structural excess | Studies show no decrease in sensitivity, with 35% reporting improved orgasm frequency |
| Cost range | Varies by treatment ($1,750 for Climax Shot, $3,995 for Morpheus8V package) | $4,900 – $9,000 depending on complexity and combination with other procedures |
| Ideal candidate | Women exploring options before committing to surgery, or those with mild functional concerns | Women with structural excess tissue, cosmetic concerns, or those combining with labiaplasty |
FormaV and VTone and other non-surgical vaginal rejuvenation options can address mild sensation concerns without incisions. If the primary issue is structural excess tissue, a surgical approach typically produces more definitive results.
What Most Resources Get Wrong About the Clitoral Hood
Most online content treats the hood as a simple flap of skin with one variable: too much or not enough. That framing misses important realities.
The hood is a dynamic structure. During arousal, the clitoral complex engorges, the hood shifts, and glans exposure changes. A hood that fully covers the glans at rest may retract significantly during arousal. Evaluating coverage only in a non-aroused state gives an incomplete picture.
Adhesions are also far more common than most women realize. Research suggests 20 to 30% of women without lichen sclerosus have some degree of clitoral adhesion. When adhesions trap keratin debris, they can cause pain, reduced sensation, or a foreign-body feeling that many women don’t connect to the hood at all.
Frequently Asked Questions
What is a clitoral hood, and what does it do?
The clitoral hood is a fold of skin at the top of the vulva that covers and protects the clitoral glans. It shields roughly 8,000 nerve endings from constant friction and allows the glans to remain sensitive to intentional stimulation during arousal.
Does the clitoral hood affect orgasm?
Yes. The hood mediates how stimulation reaches the clitoral glans. When the hood is proportionate and mobile, it facilitates a gliding sensation that contributes to arousal. Excess or thickened tissue can reduce the effectiveness of stimulation and make orgasm more difficult to achieve.
Can you have a “hooded clitoris” and still orgasm normally?
Many women with more clitoral hood coverage orgasm without any difficulty. A larger hood doesn’t automatically mean reduced function. It depends on tissue thickness, mobility, and how effectively stimulation reaches the underlying nerve endings.
What causes excess clitoral hood tissue?
Genetics is the most common factor. Hormonal changes from pregnancy, menopause, PCOS, or hormone therapy can also alter tissue volume and elasticity. Conditions like lichen sclerosus may cause the hood to thicken or adhere to the glans over time.
Is clitoral hood reduction safe?
Published studies report over 90% patient satisfaction and no decrease in clitoral sensitivity when established techniques preserve the dorsal clitoral nerve. Choosing a surgeon with training in female sexual anatomy, like a board-certified OB/GYN, is the most important safety factor.
How much does clitoral hood reduction cost at FemSculpt?
Clitoral hood reduction at FemSculpt ranges from $4,900 to $9,000, depending on complexity and whether it’s combined with other procedures. An individualized quote is provided during your consultation. Financing options through CareCredit and Cherry are available.
Can clitoral hood reduction be combined with labiaplasty?
Yes. Addressing both the labia and the hood together creates a more balanced result and avoids a second procedure. Many patients who come to FemSculpt for a labiaplasty revision specifically request hood reduction because it wasn’t done during their original surgery.
Will I lose sensation after clitoral hood reduction?
A 2015 prospective study found no decrease in clitoral sensitivity at 12 months post-procedure. Dr. Kafali’s OB/GYN background means she understands the dorsal nerve of the clitoris and plans every procedure around preserving it.
What is recovery like after hood reduction?
Most patients take about a week off work. Swelling and mild discomfort are managed with ice, elevation, and prescribed medication. Sexual activity is typically cleared at 4 to 6 weeks.
Does insurance cover clitoral hood reduction?
FemSculpt does not work with insurance companies. Patients may check with their provider to see if partial reimbursement is available for documented medical necessity.
I had a labiaplasty but my hood wasn’t touched. Can this be done separately?
Yes. This is one of the most common reasons patients seek clitoral hood reduction at FemSculpt. If your previous labiaplasty left the hood area untouched, a standalone hood reduction can address the remaining tissue and create a more proportional result.
I live out of state. Can I still have this procedure at FemSculpt?
Yes. Many FemSculpt patients travel from across the U.S. and internationally. The process starts with a $150 virtual consultation, followed by coordinated scheduling for your surgery visit. See the out-of-town patient guide for logistics.
Next Steps
FemSculpt offers virtual consultations ($150) and in-person consultations ($250) with Dr. Sue Kafali. View results in the before and after gallery, or schedule a consultation to discuss your anatomy and options. Call (312) 809-9983.
Related Content
- Clitoral Hood Reduction at FemSculpt
- Hooded Clitoris Surgery for Enhanced Pleasure
- 6 Facts About the Clitoris You Should Know
- What Is a Labiaplasty?
- Understanding Your Vulva
- Vaginal Rejuvenation Pricing
Clinical Evidence and Sources
- Herbenick, D. et al. (2018). “Women’s Experiences with Genital Touching, Sexual Pleasure, and Orgasm.” Journal of Sex & Marital Therapy, 44(2), 201-212. PubMed Survey of 1,055 U.S. women finding 18.4% orgasm from penetration alone; 36.6% require clitoral stimulation.
- Placik, O.J. & Devgan, L.L. (2015). “A Prospective Evaluation of Female External Genitalia Sensitivity to Pressure following Labia Minora Reduction and Clitoral Hood Reduction.” Plastic and Reconstructive Surgery, 136(4), 442e-452e. PubMed Prospective study of 37 subjects showing no decrease in clitoral sensitivity post-procedure, with 35.3% reporting improved orgasm frequency.
- Goodman, M.P. et al. (2010). “A Large Multicenter Outcome Study of Female Genital Plastic Surgery.” Journal of Sexual Medicine, 7(4), 1565-1577. PubMed 258-patient multicenter study: 91.6% overall satisfaction; 97.2% satisfaction for labiaplasty/hood reduction; 64.7% reported enhanced sexual function.
- Boglarka, J. et al. (2022). “The Role of Clitoral Topography in Sexual Arousal and Orgasm: Transperineal Ultrasound Study.” International Urogynecology Journal, 33(6), 1495-1502. PubMed Ultrasound study of 108 women linking clitoris-urethra distance and glans volume to orgasm function.
- O’Connell, H.E. et al. (2005). “Anatomy of the Clitoris.” Journal of Urology, 174(4), 1189-1195. Landmark anatomical study establishing the full 9-11 cm dimensions of the clitoral complex, including internal crura and bulbs.
Medical Disclaimer: The content on this page has been medically reviewed for accuracy by Dr. Sue Kafali, MD, FACOG, board-certified OB/GYN and Medical Director of FemSculpt Cosmetic Gynecology. This information is for educational purposes only and is not a diagnosis or treatment plan. Individual results vary. Candidacy, risks, and expected outcomes can only be determined after a private consultation and examination with Dr. Kafali.
*Last medically reviewed: 2026-03